
Can Fluoride Cause Colic and GI Damage?

I love “dental professional” groups on social media. They are a great place to bounce ideas off other professionals, ask questions, and, in some cases, inform each other about emerging research, new developments, products, and treatment modalities.
However, from time to time, an outlier or a professional who believes they have unearthed something that other professionals may have missed will make a bold claim. When these claims are challenged, the professional either ghost the post or deletes it.
This recently happened, and the claims were quite bold. It made me consider the fact that these claims and beliefs may be circulating in the public. Therefore, I feel like it is worth addressing.
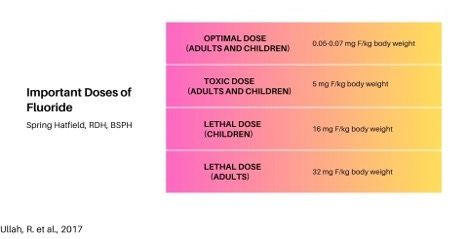
But before I address these claims, I think it is important to understand the fluoride dose-response relationship. The safe/beneficial dose, toxic dose, and lethal dose of fluoride are well established. Therefore, when assessing any claims that cite sources, check the dose used in the research. If the dose being used is in the toxic range, we would expect to see toxic results. It would be surprising if we didn’t.
Back to the claims…
The person who made these claims is, for the most part, considered a key opinion leader in dental hygiene. Because of this, I will not be calling this person out by name. I believe this person misrepresented these research results because they didn’t understand the dose-response relationship and not because they were being nefarious. I’m not trying to smear someone; I simply want to highlight how these claims are inaccurate in hopes that it will prevent the spread of this information any further.
“Did you know that when we swallow fluoride from toothpaste or in water, it changes the hydrochloric acid in our gut to hydrofluoric acid? HF acid is HIGHLY corrosive and has a detrimental effect on the microvilli lining in the stomach and intestinal walls. What if Colic is the result of ingested fluoride? Formula-feed infants’ exposure level to fluoride is 2.88 to 3.4 times greater than that of adults. (Colic is not just limited to infants.)
Fluoride can stimulate secretion of acid in the stomach (Assem and Wan 1982; Shayiq et al. 1984), reduce blood flow away from the stomach lining, dilate blood vessels, increase redness of the stomach lining (Fujii and Tamura 1989; Whitford et al. 1997), and cause cell death and desquamation of the GI tract epithelium (Easmann et al. 1984; Pashley et al. 1984; Susheela and Das 1988; Kertesz et al. 1989; NTP 1990; Shashi 2002).
What goes in the mouth doesn’t stay in the mouth. It has far-ranging effects throughout the entire body. Dentistry is only focused on one thing – tooth decay. It is time to look at the root cause of dental caries disease and while it won’t be an easy fix, we all must take responsibility for stopping the disease. Fluoride is not the healthy answer.”
There is a lot to unpack here, so let’s get to it.
Fluoride changes hydrochloric acid to hydrofluoric acid
This claim is true, yet, as usual, it is missing context. Animal studies do indicate that fluoride changes the hydrochloric acid of the stomach to hydrofluoric acid at high doses. Excessive hydrofluoric acid in these animal studies shows gastric mucosa irritation, stimulation of gastric secretions, diminished blood supply away from the stomach lining, and it can result in death of epithelial cells of the GI tract.1
However, in humans, this isn’t a problem with the levels of fluoride exposure in the U.S. There have been reports of GI issues in some countries with higher concentrations of fluoride in drinking water. This occurs with exposure of at least 3.2 ppm or higher in drinking water, not at the doses the U.S. population is exposed to through proper use of oral care products, ingestion of foods, drink, and fluoridated water.1
The references the authors cite for this claim also use high doses of fluoride in the studies. These studies are difficult to find and access, so let me give you a general idea of the ones I could access.
Shayiq et al, found intestinal permeability was observed when 4 mg/L fluoride was used, while doses of fluoride at 0.5 mg/L did not produce any significant effect. This study concluded that the change in permeability and enzymatic activity in the stomach was most probably due to high fluoride concentrations.2 The author of this claim misrepresented these findings.
In the Fujii and Tamura study, the authors found reduced blood flow away from the stomach lining, dilated blood vessels, and increased redness of the stomach lining at the dose of 300 mg/kg of body weight of fluoride. That dose is lethal in adult humans, therefore if you are exposed to a dose of fluoride that high, your stomach lining and blood vessels will be the least of your worries.3
I was unable to find several of the cited references but found that the entire section was copied verbatim from chapter 9 of the book Fluoride in Drinking Water: A Scientific Review of EPA’s Standards.
The book states, “Fluoride can stimulate secretion of acid in the stomach (Assem and Wan 1982; Shayiq et al. 1984), reduce blood flow away from the stomach lining, dilate blood vessels, increase redness of the stomach lining (Fujii and Tamura 1989; Whitford et al. 1997), and cause cell death and desquamation of the GI tract epithelium (Easmann et al. 1984; Pashley et al. 1984; Susheela and Das 1988; Kertesz et al. 1989; NTP 1990; Shashi 2002).”4
The problem is that the author stopped short of the real findings. The very next sentence states, “Because fluoride is a known inhibitor of several metabolic intracellular enzymes, it is not surprising that, at very high exposures, there is cell death and desquamation of the GI gut epithelium wall.”4
Here, we have a misrepresentation of the findings and some obvious cherry-picking.
Formula-fed infants’ exposure level to fluoride is 2.88 to 3.4 times greater than that of adults
First, let me say this is borderline lactivism, and it is not ok. There are many mothers who are unable to breastfeed for multiple reasons, implying not breastfeeding is somehow harmful is not helpful and, in my opinion, really disgusting. If you are a mother and you are formula-feeding your baby, you are doing a great job. Do not let this statement insight fear that you are somehow harming your baby; you are not.
Fed is BEST.
With that out of the way, let’s discuss this claim. It is important to understand multiple factors will determine the amount of fluoride your baby is exposed to, no matter how they are fed. Breastmilk does contain fluoride as well, although it is a negligible amount, ranging from 0.002 to 0.01 mg/L.5
Formula, depending on the type, has a fluoride content of around 0.2 mg/L. Soy formula has slightly higher doses than milk-based formulas, with doses ranging from 0.2 to 0.3 mg/L.5
For an infant being fed 2 ounces every 2 hours, that equates to approximately 0.24 mg of fluoride in a day. The tolerable upper intake level for fluoride in newborns and infants is 0.7 mg. Adults are exposed to 0.22 mg of fluoride from their morning coffee, assuming they only drink 1 cup. So, rest assured you are not exposing your baby to “2.88 to 3.4 times” more fluoride than adults.5
Colic in babies and adults
First let’s define “colic” to determine if this is a reasonable claim. The Mayo Clinic says colic is “prolonged and intense crying or fussiness in a healthy infant.”6
The cause of colic is unknown; therefore, questioning if an environmental factor could be a contributing or causal factor isn’t unreasonable. However, there is a lot to be understood about colic. For instance, why it begins late in the first month of life, why it varies among infants, why it happens at certain times of the day, and why it resolves on its own.6
The most glaring question is “why it resolves on its own.” If fluoride were the cause, then it wouldn’t resolve. It would continue until the baby was no longer exposed to the fluoride in the formula. But in most cases, colic resolves on its own, often with very little changes to the feeding routine.
Sometimes, changing from a milk-based formula to a soy-based formula resolves colic. But again, if it were the fluoride, the colic would get worse with this change since soy-based formula has more fluoride than milk-based formula. There is no evidence to support the idea that fluoride causes colic in infants.
Adults can indeed have colic, not just infants. However, in adults, it is a little better defined. Adult colic is defined as “pain in your intestinal or urinary systems.”7
There are three types of adult colic:
· Biliary colic – abdominal pain that occurs due to a blockage in a biliary duct
· Renal colic – blockage in your urinary tract; this usually causes pain between your ribs and hips
· Intestinal colic – painful cramps in the abdomen due to a blockage in your large or small intestines.7
To be fair intestinal colic can be caused by multiple things, including scar tissue, inflammatory intestinal disorders, impacted poop, and inflamed or infected diverticula. Of those causes there have been speculations about fluoride causing inflammatory intestinal disorders. But again, this is only at high doses, not the doses at which someone in the U.S. would be exposed.7,8
Dentistry isn’t focusing on the root cause
This claim is bold and, quite honestly, probably a little offensive to some dental professionals, including myself. The idea that we, as a collective whole, are not trying to identify the “root cause” of dental caries is inaccurate and could potentially damage the trust our patients have placed in us.
Dental caries are multifactorial. Often, the most significant factors are dietary habits and oral hygiene. Additionally, mouth breathing can play a huge role. Dental professionals are indeed addressing these things, among a multitude of other factors associated with increased dental caries risk.
But here is the conundrum: This post suggests we should abandon the use of fluoride because it is not “the healthy answer.” This suggests we leave our patients vulnerable to dental caries because these factors that need to be addressed take time to “fix.”
This is unacceptable. Why should we withhold a safe and effective preventive measure while we wait for vulnerable patients to modify their behavior or see an ENT to address their mouth breathing?
Just because we recommend fluoride does not indicate that we are not addressing the root cause. We are addressing the root cause while giving our patients grace. If behavior modification was easy, we would all be eating healthy and exercising daily, but we don’t. In some cases, there are barriers to that lifestyle, many of which are out of our control.
For that reason, I applaud dental hygienists who don’t cave to the pressure to join the virtue signaling of those who push to eliminate fluoride, as if every person has the same access to dental care.
Fluoride is safe and effective; it is also just as healthy a choice as other prevention modalities touted by the anti-fluoride brigade.
Conclusion
Hold on to your pants, this is a shocker… the only conclusion I can come to based on the information provided in the post is that adverse health effects associated with fluoride exposure is dose dependent.
If you have read any of my previous posts on this topic, this conclusion will be very anticlimactic. There is a theme here for a reason. We know the safe/beneficial doses of fluoride. We also know the toxic dose. When a toxic dose is used in studies, the expected outcome is adverse health effects.
The problem is that some healthcare professionals, with good intentions, fail to acknowledge these dose-response relationships and extrapolate results to apply to all doses of fluoride. That is where they make their mistake.
Any time someone makes a claim about fluoride having adverse health effects, take the time to check any references. Utilize the chart in this post to see if the doses used in the research were above the safe/beneficial dose. If so, you should expect the results to show adverse health effects.
But also, be confident in the fact that you, your children, or any other family member or friend will ever be exposed to fluoride at a toxic or lethal dose through proper use of oral health products, food, drinks, medications, or fluoridated drinking water.
References
1. Ullah R, Zafar MS, Shahani N. Potential fluoride toxicity from oral medicaments: A review. Iran J Basic Med Sci. 2017;20(8):841-848. doi:10.22038/IJBMS.2017.9104. https://pmc.ncbi.nlm.nih.gov/articles/PMC5651468/#:~:text=Gastrointestinal%20tract%20(GIT),of%20hydrofluoric%20acid%20(6).
2. Shayiq RM, Raza H, Kidwai AM. Effects of fluoride on membrane permeability and brush border enzymes of rat intestine in situ. Food Chem Toxicol. 1986;24(1):33-36. doi:10.1016/0278-6915(86)90261-9. https://pubmed.ncbi.nlm.nih.gov/2868974/
3. Fujii A, Tamura T. Deleterious effect of sodium fluoride on gastrointestinal tract. Gen Pharmacol. 1989;20(5):705-710. doi:10.1016/0306-3623(89)90111-0. https://pubmed.ncbi.nlm.nih.gov/2606338/
4. Fluoride in Drinking Water: A Scientific Review of EPA’s Standards. (2006). Chapter 9: Effects on the Gastrointestinal, Renal, Hepatic, and Immune Systems. The National Academies Press. https://nap.nationalacademies.org/read/11571/chapter/11
5. Fluoride. (2024, June 26). National Institute of Health Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/Fluoride-HealthProfessional/#:~:text=Fluoride%20levels%20can%20range%20from,are%20listed%20in%20Table%202.&text=*Amounts%20of%20fluoride%20might%20vary,prepare%20these%20foods%20and%20beverages.
6. Colic. (2022, April 5). Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/colic/symptoms-causes/syc-20371074
7. Colic. (2023, June 9). Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/10823-colic
Dionizio A, Uyghurturk DA, Melo CGS, et al. Intestinal changes associated with fluoride exposure in rats: Integrative morphological, proteomic and microbiome analyses.Chemosphere. 2021;273:129607. doi:10.1016/j.chemosphere.2021.129607.https://pmc.ncbi.nlm.nih.gov/articles/PMC8076095/#ABS1